Clinical benefits of BHI supported by 30 publications – new podcast
A PubMed search now yields 30 publications on BoneXpert’s Bone Health Index, supporting the clinical benefits of BHI.
While the gold standard for assessing children’s bone health is DEXA BMD (Dual Energy X-ray Absorptiometry Bone Mineral Density), BHI leads to five complementary benefits:
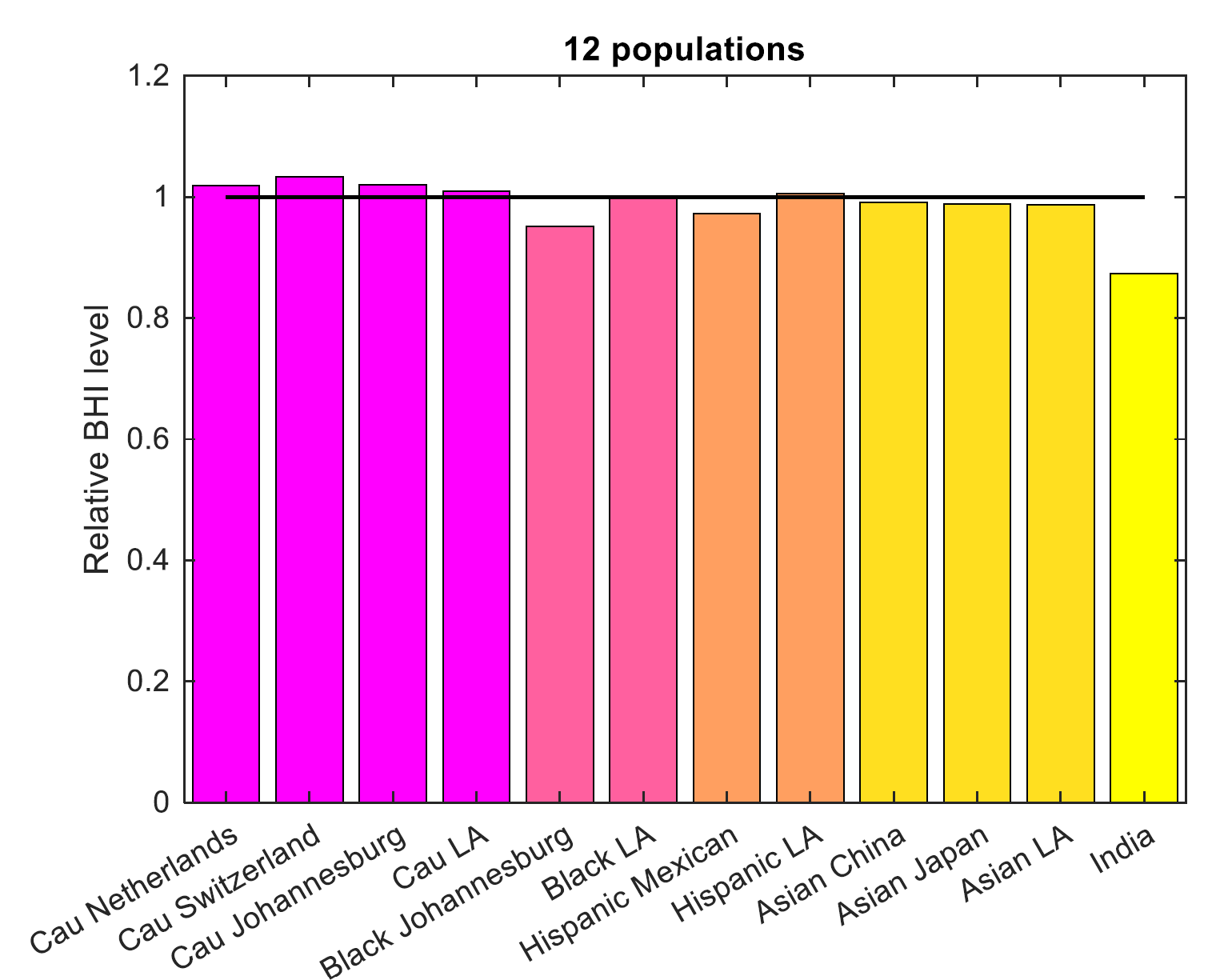
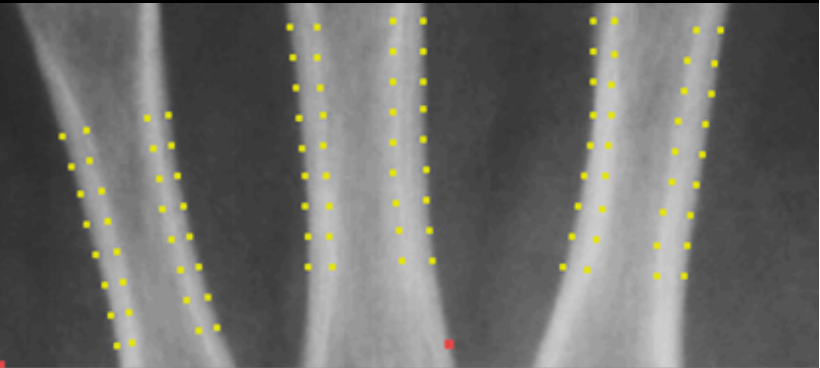
- Properly Size-Corrected: The BHI formula was designed from first principles to be intrinsically independent of children’s highly variable bone size, overcoming a major confounding factor that limits the interpretability of DEXA’s areal bone mineral density.
- Z-scores by Bone Age: BHI is fully integrated with BoneXpert’s automated bone age determination from the same X-ray, allowing for the calculation of the Z-score (called BHI SDS, Standard Deviation Score) against bone age – a more accurate measure of physiological maturity than chronological age, in particular for children with growth and puberty disorders.
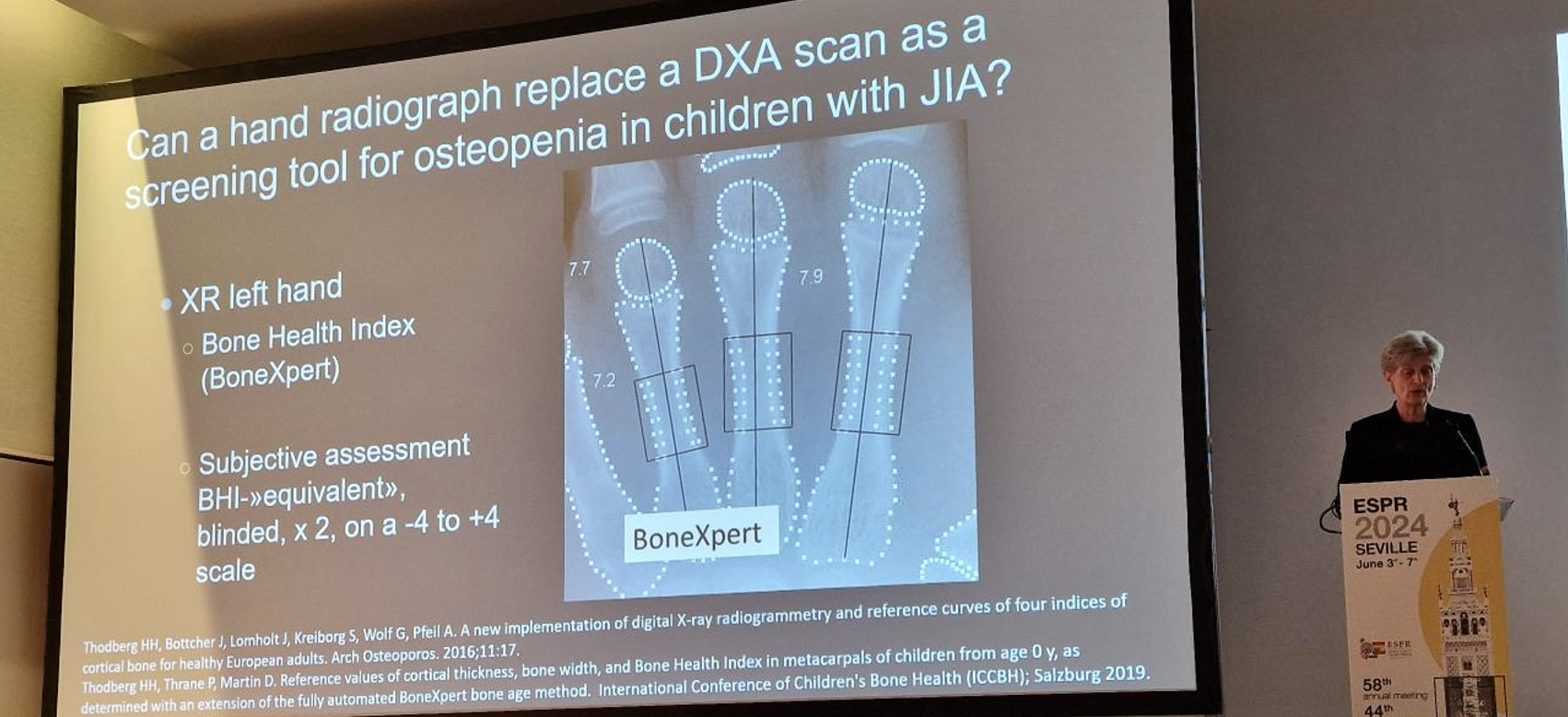
- Speed and Availability: As BHI is derived from routine bone age X-rays, it offers an opportunistic, rapid bone health assessment without additional radiation, cost, or patient visits, thereby increasing the frequency of monitoring in at-risk children.
- Clinical Validation: BHI SDS correlates with the widely used Height-Adjusted DEXA BMD Z-score (HAZ). And studies have demonstrated that a low BHI SDS is a significant predictor of fractures in high-risk populations, including children with Klinefelter syndrome, chronic inflammatory/disabling conditions and Duchenne muscular dystrophy (DMD).
- Unique Applicability: BHI is uniquely applicable in patient populations where DEXA is often impossible or unsafe. This includes children with severe physical disabilities (e.g., DMD, and cerebral palsy) due to positioning challenges and metallic implants, and children under three years of age, for whom BHI provides a sedation-free alternative to DEXA.
This podcast, generated by Notebook LM, unfolds these benefits
0:00
1:03